
Yesterday I wrote a Dutch blog article that I will translate into English soon. More than 200 scientists are now supporting the aerosol contamination theory behind COVID-19. In Holland scientist Maurice de Hond has done a fantastic job in the past months, some of his articles are already translated in English. Meanwhile read the following article from Dr Jonathan Fluxman
“In the mind of scientists working on this, there’s absolutely no doubt that the virus spreads in the air……This is a no-brainer…… We have already lost valuable time by ignoring this method of spread and we should act on the presumption that COVID-19 is spreading on the air.”
2 April 2020; Professor Lidia Morawska, International Laboratory for Air Quality and Health (ILAQH), School of Earth of Atmospheric Sciences, Queensland University of Technology, Brisbane, Australia https://www.nature.com/articles/d41586-020-00974-w
“A lot of the evidence has been pointing to aerosol transmission of respiratory viruses. …. Influenza …. SARS …… This particular virus (Covid-19), a lot of evidence is mounting……It’s just shocking to me, quite honestly, that this has not been factored in (CDC and WHO guidance).”
27 May 2020; Dr Kimberly Prather, Scripps Institution of Oceanography, University of California San Diego. https://www.webmd.com/lung/news/20200527/aerosol-scientist-covid19-is-likely-airborne (see also academic paper at reference 38)
“When you sing, the amount of droplets and aerosol that come out is really, in some respects, scary.”
26 May 2020; Dr Anthony Fauci, Director of the US National Institute of Allergy and Infectious Diseases. https://www.americamagazine.org/faith/2020/05/27/dr-anthony-fauci-catholic-churches-masks-communion-covid-coronavirus
“As long as we are sharing an airspace with someone else, breathing in the air that they exhale, airborne transmission is possible.”
2 April 2020; Dr Julian Tang Consultant Virologist at the Leicester Royal Infirmary and Honorary Associate Professor in the Department of Respiratory Sciences https://www.nature.com/articles/d41586-020-00974-w
“…..gathering unequivocal evidence for airborne transmission could take years and cost lives. We shouldn’t let “perfect be the enemy of convincing”
2 April 2020; Professor Michael T. Osterholm, Regents Professor, and Director of the Centre for Infectious Disease Research and Policy at the University of Minnesota. https://www.nature.com/articles/d41586-020-00974-w
“It’s hard to believe this pandemic could have spread the way it did so quickly around the world without the airborne route playing a role……It’s a frustration for people who understand aerosols and air pollution particles that this hasn’t received more attention. There are about a half-dozen people screaming about this from the rooftops.”
25 June 2020; Richard L. Corsi, Dean of engineering and computer science at Portland State University and a specialist in indoor air quality. https://www.firstpost.com/health/linsey-marr-solving-the-case-of-airborne-transmission-of-coronavirus-public-health-issues-with-interdisciplinary-studies-8524271.html
“Evidence is emerging indicating that, in addition to transmission via large droplets and fomites, SARS-CoV-2 is also transmitted via airborne particles. Recognition of this transmission route is critically important…….”
6 May 2020; Dr Joseph Allen Department of Environmental Health, Harvard T.H. Chan School of Public Health, Boston and Professor Linsey Marr, Charles P. Lunsford Professor of Civil and Environmental Engineering at Virginia Tech; Blacksburg VA USA https://www.preprints.org/manuscript/202005.0126/v1
“Risk of aerosol transmission is highest when people share poorly ventilated spaces where the viral aerosols can build up.……. Transmission by aerosol can happen at distances beyond 2m in the same enclosed space especially if the ventilation is poor and duration of exposure is sufficient…….. prevention and mitigation measures….. “should consider all of the known transmission routes together with the time that someone is exposed.”
4 June 2020; Environmental Monitoring Group, report to the UK Scientific and Advisory Group for Emergencies (SAGE). https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/892043/S0484_Transmission_of_SARS-CoV-2_and_Mitigating_Measures.pdf
More than 200 scientists from around the world are challenging the official view of how the coronavirus spreads…..(in) open letter to the WHO to be published next week …… accusing the United Nations agency of failing to issue appropriate warnings about the risk. A total of 239 researchers from 32 countries signed the letter…..
They say multiple studies demonstrate that particles known as aerosols …… can hang in the air for long periods and float dozens of feet, making poorly ventilated rooms, buses and other confined spaces dangerous, even when people stay six feet from one another.
4 July 2020; Richard Read, Los Angeles Times. https://www.latimes.com/world-nation/story/2020-07-04/coronavirus-airborne-spread
1. Introduction
This emotional language from some of the world’s top experts in airborne transmission of diseases and the behaviour of aerosolised viruses, is testimony to the desperation and frustration currently felt by many towards the world’s leading public health bodies, over their failure to recognise airborne spread of Covid-19. The failure of WHO, CDC and Public Health England to accept that this and therefore to advise how to combat airborne spread, continues to put people at risk all over the world. The stakes could not be higher: the pandemic is accelerating, especially in the global south, with over 10 million reported cases and 500,000 deaths. But as we confront the pandemic, we find ourselves hamstrung by this guidance, unable to rely on it to protect our families, communities, workplaces and indoor public spaces.
Like many, here in the UK we are at a critical moment in the battle against Covid-19. We have already paid a very heavy price, with total excess mortality put at over 65,700 on 22 June 2020. (1) We are opening up pubs, bars, restaurants and shops, many people will gather in these indoor, often poorly ventilated spaces, while at the same time the government has relaxed social distancing rules. There is still significant viral transmission in the community, (the best estimates are between 2,300 and 4,300 new infections per day as of 20 June. (2)), and local outbreaks emerging. Not surprisingly there is widespread concern about this from a range of experts (3), as well as deep unease among large sections of the public.
This article looks at the guidance of Public Health England (PHE), the US Centre for Disease Control (CDC) and the World Health Organisation (WHO), which are all similar, as well as that of the European Centre for Disease Control, which is quite different. We will also look at some landmark studies in the transmission of Covid-19, and examples of airborne spread in two enclosed environments, i.e. on buses and in meat processing plants.* In the reference section there are listed a number of other important studies with brief descriptions of their findings. These are not referenced in the body of this article, but add to the weight of evidence for aerosol spread.
There is a link at the end of this document (and here), to an open letter addressed to the heads of WHO, CDC and PHE. It calls on them to urgently review their guidance on transmission of Covid-19. If you agree please add you name and share with others. Thank you.
* For a discussion about how the various factors involved in virus transmission relate to a wide range of day-to-day activities please see this companion article here:
CONTENTS
1. Introduction
2. How does indoor aerosol spread occur
-
Covid-19 is an indoor disease
-
How aerosols are generated
-
Videos showing airborne spread
-
Aerosol route of infection may be more dangerous
-
PHE, CDC and WHO say no aerosol spread
3. Public Health England (PHE) guidance on transmission
-
Covid-19 and SARS similarities in transmission
-
Aerosol generating procedures (AGPs)
-
Evidence from government scientific committee reports
-
A word about evidence and Covid-19
4. CDC guidance on transmission
5. WHO guidance on transmission
6. European CDC guidance on transmission
7. Reports of specific outbreaks events of Covid-19
-
Choir in Washington State
-
Restaurant in Guangzhou
-
Call centre in Seoul
-
Bus drivers in London
-
Bus passengers Zheziang
-
Meat and poultry processing plants
8. Face coverings
9. Conclusion
10. Open letter to WHO, CDC and PHE
11. Other publications and reports
12. References
2. How does aerosol spread occur?
Covid-19 is an indoor disease
Covid-19 transmission occurs indoors the great majority of the time, (4) so it is important to have a good understanding of how the virus spreads in enclosed spaces if we are to keep safe. We know about contact spread, either by touching each other, or touching surfaces contaminated by live virus and then our faces; hence the need to wash our hands frequently. We also know about “droplet” spread – these are moisture droplets produced when we breathe out, which contain the virus, and which can infect people close by. These large droplets fall quickly to the floor within 1-2m, hence the 2m rule for social distancing.
However, the harder and deeper we breathe the more virus we produce, so talking, laughing, singing, shouting, exercising, coughing and sneezing generate increasing amounts of virus and project these large droplets over bigger distances. The speed of airflow has been estimated with different activities: quiet breathing up to 1 m/s; talking 5 m/s; coughing 2–50 m/s; and sneezing > 100 m/s. (5) Its estimated that a single cough from an infected individual can project large numbers of virus particles into the air over a distance of several metres. (6)
How aerosols are generated
There is another type of spread through the air, in addition to large droplets. The diagram below illustrates this quite well. Note that in addition to the larger droplets which fall to the floor, and the big distances involved when we cough and sneeze, a range of droplet sizes are produced from large droplets to extremely small ones, which are known as “droplet nuclei”. All of these contain live virus. The smallest are also known as virus aerosols and do not fall to the ground straight away, but can remain suspended and infectious in the air for anything from 15 minutes up to 3 hours. (9) (10)
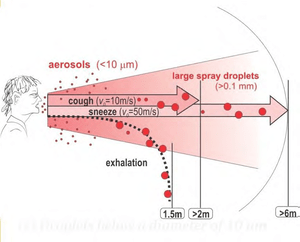

Figure 1 Spread of Covid-19 by droplets and aerosols (with thanks to the One Heart Clinic https://www.oneheartclinic.com/) Aerosols are created when talking, shouting, laughing, singing, exercising as well as when coughing and sneezing.
Its important to understand that whenever we breathe out a range of droplets is produced including aerosolised virus. If we are breathing quietly small amounts are produced, more with talking (9), still more with laughing, singing or shouting, and large numbers from coughing and sneezing. It is not known for certain which sizes of droplets predominate when we breathe out, but the Environmental Monitoring Group, which reports to SAGE (SAGE advises UK government ministers on the science of the pandemic), stated in a report on 28 April 2020, that “the majority of recent studies (in the laboratory) suggest most particles are below 10mm”, i.e. the size of aerosolised virus particles. (11)
Because aerosolised viruses are suspended in the air, (like the dust particles that can be seen floating in the air in the sunlight after dusting a room), it means they can travel over longer distances and fill enclosed spaces. The infective dose for Covid-19 is estimated to be about a thousand virus particles (7) (8), so an infected person coughing or laughing in an enclosed indoor space can potentially infect everyone in that space if they spend much time there. The 2m rule will therefore not be protective. If the air is stagnant with poor ventilation, virus- containing aerosols will fill the whole indoor space over a period of time. The smaller the space the quicker it will fill with virus; a large space will take longer, but as we will see later. even large indoor spaces, like call centres and meat packing plants, can become “aerosol rich environments”, exposing everyone in that space to potential infection. This concept is important to bear in mind.
Videos showing airborne spread
These two videos, from Japan and the US, demonstrate airborne spread quite well, both larger droplet spread and aerosol spread.
https://youtu.be/vBvFkQizTT4 (see from 4 min 20 secs in particular)

https://youtu.be/ZQKEHBFI9uE


Ventilation is therefore very important.If there are sufficient windows, allowing for cross draughts and sufficient exchange of air in the room, an aerosol rich environment will not be created and the space will be much safer.However, the pattern of airflow is important, people sitting downwind in the airstream from an infected person can still get infected.One small window in a room, or air conditioning which warms or cools by circulating room air, or a fan, will not clear virus from the air, and everyone in the room will remain at risk.Room air must be exchanged by ventilation, not simply re-circulated, to clear aerosolised virus.
The aerosol route of transmission of Covid-19 clearly has major implications for control measures to try and contain the virus and prevent spread. The practical difficulties of ensuring adequate ventilation in the many thousands of shops, offices, pubs and restaurants are such that it is not possible to make very many of these indoor spaces “covid safe”. The problem is greatly increased by the lack of awareness among the public and business owners of aerosol spread; increased spread is therefore highly probable as restrictions are lifted and control measures weakened as we have seen elsewhere, for example in the southern United States recently.
Aerosol route of infection may be more dangerous
This is a further worry. Because the droplet nuclei are so small they are inhaled deep into the lungs when breathed in, straight to the alveoli (air sacs) which have fewer defences against infection. Larger droplets can be filtered out in the nose and some will be trapped in the larger upper airways and not penetrate into cells. There is evidence for the influenza virus that aerosol infection can cause more severe disease, lower (rather than upper) respiratory infection, and may cause infection even with a one-hundred-fold lower viral dose. (5)
Official guidance on transmission of Covid-19
Let us now turn to the official guidance about transmission of Covid-19. The World Health Organisation (WHO), the US Centre for Disease Control (CDC) and Public Health England
(PHE) do not accept that aerosol spread of Covid-19 occurs, except in hospitals for some strictly defined medical procedures, and therefore do not need taking precautions against. The European Centre for Disease Control (ECDC) differs significantly in this; we’ll discuss this shortly.
It is not clear why these leading health bodies dismiss aerosol spread in the face of increasingly convincing evidence from a variety of sources. They also fail to take into account reports, which the governments of the USA and UK have themselves commissioned from their own scientific committees. The reports clearly identify aerosol spread as a serious risk and advise that countermeasures such as face masks and improved ventilation should be implemented against it. As we have seen there is growing frustration and dissatisfaction from scientists and medical experts at this situation.
3. Public Health England (PHE) guidance on transmission
PHE guidance, updated on 18 June 2020, (11) states:
“Infection control advice is based on the reasonable assumption that the transmission characteristics of COVID-19 are similar to those of the 2003 SARS-CoV outbreak. The initial phylogenetic and immunologic similarities between COVID-19 and SARS-CoV can be extrapolated to gain insight into some of the epidemiological characteristics.
The transmission of COVID-19 is thought to occur mainly through respiratory droplets generated by coughing and sneezing, and through contact with contaminated surfaces. The predominant modes of transmission are assumed to be droplet and contact.
During aerosol generating procedures (AGPs) there is an increased risk of aerosol spread of infectious agents irrespective of the mode of transmission (contact, droplet, or airborne), and airborne precautions must be implemented when performing (these), including those carried out on suspected as well as confirmed cases of COVID-19.
Initial research has identified the presence of COVID-19 virus in the stools and conjunctival secretions of confirmed cases. All secretions (except sweat) and excretions, including diarrhoeal stools from patients with known or possible COVID-19, should be regarded as potentially infectious.”
This can be summarised as the following; we will discuss the points below:
-
SARS-CoV2 (Covid-19) is sufficiently similar to SARS-CoV1 (which caused the SARS outbreak in 2003), that it is reasonable to assume they share transmission characteristics.
-
Covid-19 is spread mainly by droplets and contact with contaminated surfaces (no mention of aerosol spread).
-
Aerosol spread only applies to certain medical and dental “aerosol generating procedures”. These include things like intubating patients (inserting a tube in the windpipe), ventilation, high speed dental drills etc.
-
There may be risk of spread from faeces and other body fluids. (There are no reports of confirmed cases via this route of spread so far, so this will not be discussed further.)
Covid-19 and SARS similarities in transmission
A study in the New England Journal of Medicine (NEJM), which analysed 187 cases of SARS in the Amoy Gardens housing complex in Hong Kong in 2003, found,
“Residents of the floors at the middle and upper levels in building E were at a significantly higher risk than residents on lower floors; this finding is consistent with a rising plume of contaminated warm air in the air shaft generated from a middle-level apartment unit.” The study concluded: “Airborne spread of the virus appears to explain this large community outbreak of SARS, and future efforts at prevention and control must take into consideration the potential for airborne spread of this virus.” (12)
Another study in the NEJM of an outbreak of SARS on an aircraft, caused by one infected person (the index patient) on a flight in 2003, found,
“Illness in passengers was related to the physical proximity to the index patient, with illness reported in 8 of the 23 persons who were seated in the three rows in front of the index patient, as compared with 10 of the 88 persons who were seated elsewhere”.
The authors also say that while other routes of infection such as close contact between passengers may have been possible:
“90 percent of the persons who became ill were seated more than 36 in. (1 metre) away from the index patient, so airborne, small-particle, or other remote transmission may be more straightforward explanations for the observed distribution of cases.“ (13)
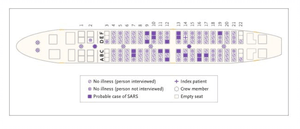

Diagram of the Boeing 737-300 Aircraft on 3 hour flight from Hong Kong to Beijing 15 March 2003 showing distribution of cases of SARS. Index patient [+] is at the middle seat on right hand side aisle 14. With thanks to Olsen et al, NEJM: https://www.nejm.org/doi/full/10.1056/nejmoa031349
In its SARS 1 Basics Fact Sheet the US CDC says, “it is possible that the SARS virus might spread more broadly through the air (airborne spread).” (14)
So, if airborne transmission of SARS is recognised, and SARS and Covid-19 are similar enough to share transmission characteristics, why is it not included as a possible transmission route for Covid-19 in PHE guidance?
Aerosol generating procedures (AGPs)
A number of medical procedures and use of some dental equipment are known to generate aerosols in the room air around patients having these procedures done. These AGPs include things like ventilation, intubation, airway suctioning and bronchoscopy. There is a list here: [https://www.rdash.nhs.uk/wp-content/uploads/2017/08/Appendix-46-Aerosol-Generating-Procedures.pdf.] There are very specific protection measures against Covid-19 that must be taken by health care staff when performing AGPs, as well as strict cleaning regimens and ventilation requirements (15) to make rooms safe following AGP procedures.
It does not make sense however, why some procedures, for example patients undergoing intubation (inserting a tube into the windpipe), are accepted as generating aerosols, yet patients who are breathing hard and coughing due to Covid-19 infection are not considered to be generating virus-rich aerosols in the air around them. The risk to health care professionals during intubation, is that the airway will be stimulated, provoking coughing by the patient, with doctors and nurses very close by being at high risk. That is one of the reasons why patients are given muscle relaxing drugs just prior to intubation, the induced paralysis will prevent any cough. So the risk is from coughing, there is nothing else in the process which can conceivably generate an aerosol. Therefore, how is this different from an awake patient coughing and breathing hard from a Covid-19 viral pneumonia? The work of breathing surely determines how much virus is expelled both as droplets and aerosols.
An excellent narrative review article published by Wilson et al in the Journal of Anaesthesia on 20 April 2020 on airborne transmission of Covid-19 to health workers, discusses this in detail. The article summary states:
“The evidence defining aerosol-generating procedures comes largely from low-quality case and cohort studies where the exact mode of transmission is unknown as aerosol production was never quantified. ……….. There is no proven relation between any aerosol-generating procedure with airborne viral content with the exception of bronchoscopy and suctioning. The mechanism for severe acute respiratory syndrome coronavirus-2 (Covid-19) transmission is unknown but the evidence suggestive of airborne spread is growing. We speculate that infected patients who cough, have high work of breathing, increased closing capacity and altered respiratory tract lining fluid will be significant producers of pathogenic aerosols. We suggest several aerosol-generating procedures may in fact result in less pathogen aerosolisation than a dyspnoeic and coughing patient.” (5)
Its also interesting to see what the authors say about aerosol spread itself:
“Three mechanisms have been described for the production of smaller sized respiratory particles (‘aerosols’) that, if inhaled, can deposit in the distal airways. These include: laryngeal activity such as talking and coughing; high velocity gas flow; and cyclical opening and closure of terminal airways. Sneezing and coughing are effective aerosol generators, but all forms of expiration produce particles across a range of sizes.”
So all types of breathing and respiratory effort produce virus containing aerosols and some of the AGPs produce less aerosol virus than a patient who is breathless and coughing. They conclude that while the exact mode of transmission is still controversial “as was the case with SARS-CoV-1 and influenza”, in the meantime we should take a precautionary approach against aerosol spread until robust evidence is available.
They summarise the balance of evidence for aerosol/airborne transmission in this diagram:
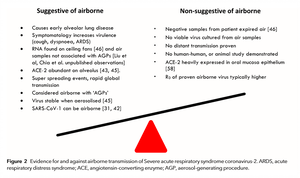

With thanks to Wilson et al; Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: a narrative review. Anaesthesia; 8 May 2020 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7264768/
Evidence from government scientific committee reports
The third issue which undermines current PHE advice is that it has ignored on several occasions detailed submissions from one of the government’s own expert sub-committees on routes of transmission. The Environmental Monitoring Group (EMG)* is one of seven sub-committees which report to SAGE, which in turn advises government ministers on the pandemic. A report dated 14 April 2020 (16) agrees with and discusses in some detail the information presented above, including the range of airborne droplets produced during breathing and coughing, the importance of indoor vs outdoor environments, and the need for ventilation. One of the recommendations of this report is:
There are environmental control strategies such as building ventilation where it may be prudent already to give stronger recommendations as a precautionary measure, particularly in higher risk enclosed environments. Providing clearer guidance on how people could do this in different environments would be useful.”
* The purpose of the EMG (also referred to as the Environmental Working Group) is “to identify and steer the role that environmental modelling, data analysis and environmental sampling can play in understanding COVID-19 transmission, with a view to understanding transmission routes, factors that influence this and the impact of environmental and behavioural interventions and mitigations at a mechanistic level.” https://www.gov.uk/government/publications/scientific-advisory-group-for-emergencies-sage-coronavirus-covid-19-response-membership/list-of-participants-of-sage-and-related-sub-groups#environmental-working-group
Another report dated 28 April by EMG to SAGE (17) refers repeatedly to “the three transmission routes”. Paragraph 14 states: We have considered transmission through airborne (inhalation), droplet and contact routes, and mitigation measures for these; however it should be noted that the relative importance of these three routes is unknown and may vary with the setting and the infectious person. The evidence to date suggests it is highly likely that short range droplet/aerosol and contact transmission dominate in most settings.”
Paragraph 16 discusses the importance of time spent in an infectious environment: “For all transmission routes, the longer an infectious person spends in an environment, the greater the contamination they will leave in that environment for others to come into contact with. Laboratory studies demonstrate that surface contamination could persist for over 72 hours, although there is a substantial reduction after 48 hours. Although the virus has been shown to survive in the aerosol state, any aerosol particles (< 5 mm diameter) are unlikely to persist at a significant level for more than 30 minutes unless the ventilation is very poor”.
Paragraph 20 states: “Improving ventilation is highly likely to have the greatest effect on airborne exposure in poorly ventilated environments with high occupant density, and increasing fresh air change rates is recommended where practical.”
Another EMG report dated 12 May 2020 (18) to SAGE concerns spread in hospitals and recommends that surface contact (touch) transmission should be considered important in hospitals. It also advises careful use of available space, for example using a corridor as a patient waiting area may be risky as “Ventilation/airflows in a corridor may disperse virus aerosols posing an infection risk, including to others who have to use the corridor”.
A further EMG report dated 4 June 2020 (19) considered transmission of Covid-19 and mitigating measures. This report also repeatedly refers to the “three transmission routes” (close range droplet spread, surface contact spread and aerosol spread). It describes in considerable detail the different types of spread, and states that prevention and mitigation measures, “should consider all of the known transmission routes together with the time that someone is exposed.” (their emphasis)
The EMG report contains this illustration of transmission routes of Covid-19. Note the distance measure along the bottom of the diagram.


Later on the report says, “Risk of aerosol transmission is highest when people share poorly ventilated spaces where the viral aerosols can build up rather than being diluted and removed by the ventilation. Risk increases with time spent in the same shared air. Risk is generally higher closer to the infectious person, but beyond this close proximity the concentration of aerosols that a susceptible person will be exposed to depends on the ventilation in the room. Transmission by aerosol can happen at distances beyond 2m in the same enclosed space especially if the ventilation is poor and duration of exposure is sufficient. It is possible but unlikely that aerosol transmission can happen between people in different rooms (via ventilation systems). Aerosol transmission risk is considered to be very low outdoors due to high dilution of virus carrying aerosols and UV inactivation of the virus.”
Current PHE guidance includes none of this, for reasons unknown. Its failure to mention aerosol spread as a threat in the community, workplaces, shops, restaurants and pubs, and what can be done to prevent it, makes the guidance unfit for purpose and puts us all at risk. The guidance requires urgent revision, especially that the country is embarking on further easing of lockdown and there will be much greater mixing of people in enclosed indoor spaces.
A WORD ABOUT EVIDENCE AND COVID-19
This dreadful pandemic is new for all of us, members of the public, health professionals and experts alike. We know more now, 6 months into the pandemic than we did at the beginning but there are still big gaps in our knowledge, and we have little in the way of effective treatment and as yet no vaccine.
In medicine and science generally, we are guided by evidence, i.e. facts proven to be true by scientific method and “peer reviewed” (checked) by experts, to verify they are true and can be relied upon. Evidence can be high quality (eg from systematic reviews of randomised controlled trials [RCTs]) or low quality (eg from observational studies). There are various ways of assessing evidence; the Centre for Evidence Based Medicine (CEBM) in Oxford has a helpful guide to levels of evidence, (20) while the GRADE system (21) allows researchers to communicate to others the reliability of the recommendations they are making, for example high confidence, moderate, low or very low confidence.
Ideally we would want to be guided by high quality evidence, for every intervention we make, but this is not always possible, and Covid-19 poses particular challenges in this regard. It is a highly infectious deadly pathogen so RCTs are very difficult – we cannot deliberately expose one group of people to the virus and compare them to another, control group, which has not been exposed. That is one reason why there has been so much debate about the evidence during the pandemic. Another is the difficulty of studying a new virus which spreads in a variety of ways, including by people who are asymptomatic, and which is deadly to older people but miraculously spares most children.
Because of these challenges we find ourselves sometimes having to make decisions, policies and interventions based on weak, limited, or even no direct evidence. “Weak” evidence is sometimes mistaken to mean the evidence is zero or wrong. It does not mean those things, instead it means there is some, limited evidence so far (see also absence of evidence below). So we may have to act according this limited evidence, especially in situations of great urgency, and include logic and our best judgement of what we think might work. There is also the “precautionary principle”, which means essentially “better safe than sorry”, which sometimes needs to be the deciding factor about an intervention, in the absence of clear evidence either way. Proponents of face coverings for example used this in arguments in favour of their use, because it was felt there was little evidence of harm and potentially much benefit from them.
If we look at the three likely routes of spread of Covid-19, there is no systematic review of the evidence that confirms the virus spreads in the ways we think it does. And when we look at the interventions we have put in place like the 2m social distancing rule [now “1m plus”], handwashing and use of face masks, there is similarly no gold standard body of evidence for any of them. If we take handwashing for example, there are no studies that confirm that this is effective in reducing contact spread of Covid-19 itself; we rely instead on evidence that handwashing kills bacteria, it is effective against SARS 1, and a study in 2001 which showed it reduced respiratory infections in soldiers. (22) Does it work against Covid-19? Almost certainly yes, that’s why we all do it. The 2m rule is based on what is known about large droplet behaviour in general, and what happens with other respiratory pathogens. There is no RCT evidence, nor are we likely to get it; but we adopt the rule because it makes sense, fits what evidence there is and appears to work.
Absence of evidence is not evidence of absence
This is an old saying in science, which means because we don’t have evidence for something, it does not mean that thing does not exist or does not occur. We saw this played out over many weeks here in the UK in relation to the wearing of face coverings by the public to reduce spread of Covid-19. The government repeatedly said this was not advisable because “the evidence was weak”. Yes, there was no high quality direct evidence but there was a very large amount of supporting evidence from other countries as well as the general principles of physics applied to air flow etc, pointing to likely benefit. For reasons which remain unknown, the government did not accept they would be helpful until late April when it relented and said they were a good idea. Face coverings were made compulsory on public transport on 15 June, and are now being promoted by the government as one of the essential measures to enable us to safely reduce social distancing to “1m plus”.
We see similarities with what is happening in relation to aerosol spread of Covid-19. No gold standard evidence exists for it but everything we do know about viral transmission of respiratory diseases, what we have seen about patterns of spread of the virus, the general principles of the physics of air flow and our logic and good judgement indicates that it is very likely. And once again the precautionary principle should apply, i.e. we should intervene to reduce aerosol spread because of the incredibly high stakes involved.
The EMG takes a similar view when it stated on 4 June that “Decisions on selection of engineering controls will inevitably need to be based on incomplete evidence as “do nothing” is not an option. Appropriate controls should be identified through collaborative risk assessments carried out between employers and employees.” It also made a “high confidence” recommendation that “Selection of prevention and mitigation measures should consider all the potential transmission routes (i.e. including aerosol spread) and need to be bespoke to a setting and the activities carried out.” (19) (emphases added)
4. CDC GUIDANCE ON TRANSMISSION
This was updated on 16 June 2020 and reads as follows:
COVID-19 is thought to spread mainly through close contact from person-to-person. Some people without symptoms may be able to spread the virus. We are still learning about how the virus spreads and the severity of illness it causes.
Person-to-person spread
The virus is thought to spread mainly from person-to-person.
· Between people who are in close contact with one another (within about 6 feet).
· Through respiratory droplets produced when an infected person coughs, sneezes, or talks.
· These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs.
· COVID-19 may be spread by people who are not showing symptoms.
The virus spreads easily between people
How easily a virus spreads from person-to-person can vary. Some viruses are highly contagious, like measles, while other viruses do not spread as easily. Another factor is whether the spread is sustained, which means it goes from person-to-person without stopping.
The virus that causes COVID-19 is spreading very easily and sustainably between people. Information from the ongoing COVID-19 pandemic suggests that this virus is spreading more efficiently than influenza, but not as efficiently as measles, which is highly contagious. In general, the more closely a person interacts with others and the longer that interaction, the higher the risk of COVID-19 spread.
So, again, no mention of airborne or aerosol spread. All of the arguments made above in relation to PHE advice would also apply to the CDC’s advice. And like PHE, the CDC also appears to be ignoring advice from an official government expert committee. Below is a letter from an expert committee on infectious diseases to Dr. Kelvin K. Droegemeier, Director of The White House Office of Science and Technology Policy, (a position like that of the Chief Scientific Advisor here in the UK). The letter is a summary of a report requested by Dr Droegemeier:
April 1, 2020
Dear Dr. Droegemeier:
This letter responds to your question concerning the possibility that SARS-CoV-2 could be spread by conversation, in addition to sneeze/cough-induced droplets.
Currently available research supports the possibility that SARS-CoV-2 could be spread via bioaerosols generated directly by patients’ exhalation.
Additional research specific to the aerosolization of SARS-CoV-2 during breathing and speech, the behavior of SARS-CoV-2 containing aerosols in the environment, both from laboratory studies and clinical experience, and the infectivity of bioaerosols containing SARS-CoV-2, would provide a more complete understanding of the level of risk of transmission of SARS-CoV2 via bioaerosols spread by exhalation and normal speech. However, for no respiratory virus is the exact proportion of infections due to air droplet, aerosol, or fomite transmission fully established, and many individual factors and situations may contribute to the importance of each route of transmission.
While the current SARS-CoV-2 specific research is limited, the results of available studies are consistent with aerosolization of virus from normal breathing.
My colleagues and I hope this input is helpful to you as you continue to guide the nation’s response in this ongoing public health crisis.
Respectfully,
Harvey V. Fineberg, M.D., Ph.D.
Chair, Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats (23)
So again we see a statement from an expert group that there are three different methods of spread including the fact that aerosols are produced with normal breathing.
Another paper dated 1 June 2020 in the Journal of the American Medical Association (JAMA) suggests that the response by Dr Fineberg’s expert group “likely contributed to the recommendation from the US Centers for Disease Control and Prevention (CDC) that healthy persons wear nonmedical face coverings, when in public, to reduce virus spread from undiagnosed infectious cases.” (24)
Again the question needs to be asked, why does CDC not include airborne spread in its guidance on transmission of Covid-19?
5. WHO GUIDANCE ON TRANSMISSION
WHO guidance was last updated on 29 March 2020, i.e. 3 months ago; what follows are extracts from the guidance: (25)
Respiratory infections can be transmitted through droplets of different sizes: when the droplet particles are >5-10 μm in diameter they are referred to as respiratory droplets, and when then are <5μm in diameter, they are referred to as droplet nuclei. According to current evidence, COVID-19 virus is primarily transmitted between people through respiratory droplets and contact routes. …….
Airborne transmission is different from droplet transmission as it refers to the presence of microbes within droplet nuclei, which are generally considered to be particles <5μm in diameter, can remain in the air for long periods of time and be transmitted to others over distances greater than 1 m.
In the context of COVID-19, airborne transmission may be possible in specific circumstances and settings in which procedures or support treatments that generate aerosols are performed; i.e., endotracheal intubation, bronchoscopy, open suctioning, administration of nebulized treatment, manual ventilation before intubation, turning the patient to the prone position, disconnecting the patient from the ventilator, non-invasive positive-pressure ventilation, tracheostomy, and cardiopulmonary resuscitation. (i.e. AGPs)
The guidance then goes on to consider findings of COVID-19 virus in air sampling as evidence of airborne spread, but rejects this on the grounds that these were only in experimental conditions and “(do) not reflect a clinical setting”; and “the detection of RNA is not indicative of viable virus that could be transmissible”.
The WHO concludes by saying that their guidelines are consistent with “other national and international guidelines, including those developed by the European Society of Intensive Care Medicine and Society of Critical Care Medicine14 and those currently used in Australia, Canada, and United Kingdom.
It also says however “At the same time, other countries and organizations, including the US Centers for Diseases Control and Prevention and the European Centre for Disease Prevention and Control, recommend airborne precautions for any situation involving the care of COVID-19 patients…” i.e. not only during AGP’s.
We have dealt with the issue of AGPs in detail above, and shown that the assertion that aerosols are only produced during AGPs in hospitals does not stand up. The WHO’s rejection of experimental evidence in the lab (the 3-jet collision nebuliser study published in the NEJM (26)) as having no relevance to clinical practice, is puzzling. Yes, it is an artificial environment but the findings are worrying – live virus particles remained suspended in the air for up to 3 hours. To simply rule out the possibility of aerosol spread because it is not in a clinical setting is not helpful, a more balanced view needs to be taken. More so given what we have said about the difficulties conducting studies with this deadly virus in real life settings. In fact, the NEJM paper has 774 citations to date (30 June 2020) by other scientists and researchers, so it seems to have the confidence of the international scientific community.
The WHO guidance does acknowledge that the US CDC and the ECDC advise precautions against aerosol spread for health care staff with any Covid-19 patient, not just those undergoing AGPs.
Wilson et al in their paper in Anaesthesia referred to above (5), take issue with another aspect of WHO guidance, i.e. the WHO’s “simple dichotomy” of airborne droplets into those less than 5um and those greater than 5um:
“The WHO 5-um size threshold used to differentiate droplet from airborne transmission is an over-simplification of the multifactorial mechanisms governing aerosol dispersal and deposition…… ..Rather than defining an exact 5-um diameter cut-off to define droplet or aerosol spread, lung particle deposition should be considered a continuum under which variables define the risk of lung deposition.”
They demonstrate the many factors involved in aerosol transmission from an infected patient breathing normally, to healthcare workers in the diagram below.
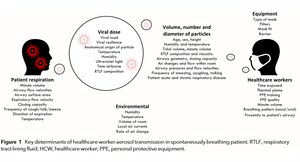

While some of this is quite technical, the bottom line is that conscious awake patients (and therefore people generally) produce airborne particles of a whole range of sizes, from large droplets to tiny airborne droplet nuclei, and risks of infection relate to the work of breathing, time of exposure and distance from the infected person.
Another excellent paper, by Allen and Marr dated 5 May 2020 in Preprints, also takes issue with WHO on the division of particles simply into smaller or greater than 5um, in the section on aerosol physics:
While the traditional distinction between “droplet” and “airborne” transmission of infectious disease has been useful for setting guidelines on the use of personal protective equipment, it has also established a false dichotomy in understanding the behavior of viruses in the air. Virus-containing droplets that are released by breathing, talking, and coughing span a continuum of sizes, from 0.01 to hundreds of microns. It is impossible for someone to release “large droplets” (>5 microns) without also releasing smaller ones. Thus, transmission that is purported to occur via the spray of large droplets from a cough could in fact be occurring through inhalation of much smaller droplets at close range. In fact, a physics-based simulation suggests that the majority of exposure at close range occurs by inhalation of small droplets rather than by contact with large droplets that land on the mouth, nose, and eyes, unless the people are closer than 30 cm or the droplets are very large.” (46) (The EMG report said the same thing about which size droplets may predominate during spread)
In the light of the accumulating evidence of this and many other papers, articles and opinions in the last 3 months, surely it is time to change WHO guidance on transmission.
6. EUROPEAN CDC GUIDANCE ON TRANSMISSION
This is quite different, it clearly accepts that aerosol transmission is very likely, as the following extracts from the 11 June 2020 update of the guidance show. (27) [It is interesting to note what it says about fomite (contact) spread, in contrast to the much greater emphasis placed on this route by PHE and CDC].
The ECDC guidance is reproduced at length here, in part because it discusses some of the landmark studies pointing to aerosol transmission, and also to demonstrate its more balanced approach to this issue.
“Infection is understood to be mainly transmitted via large respiratory droplets containing the SARS-CoV-2 virus. Transmission through aerosols has also been implicated but the relative role of large droplets and aerosols is still unclear. Indirect transmission through fomites that have been contaminated by respiratory secretions is considered possible, although, so far, transmission through fomites has not been documented……
Crowded and confined indoor spaces
Several outbreak investigation reports have shown that COVID-19 transmission can be particularly effective in crowded, confined indoor spaces such as workplaces including factories, churches, restaurants, ski resorts, shopping centres, worker dormitories, cruise ships and vehicles, or events occurring indoor such as, parties, and dance classes. They indicated that transmission can be linked with specific activities, such as singing in a choir or religious services that may be characterised by increased production of respiratory droplets through loud speech and singing.
In a study of 318 outbreaks in China, transmission in all cases except one occurred in indoor spaces. The only case of outdoor transmission identified in this study involved two persons. However, outdoor events have also been implicated in the spread of COVID-19, typically those associated with crowding such as carnival celebrations and football matches suggesting a risk of transmission linked to crowding even at outdoor events. However, exposure in crowded indoor spaces is also very common during such events.
The duration that people stay in indoor settings appears also to be associated with the attack rate. For example, in a 2.5 hour choir practice in Washington, US, there were 32 confirmed and 20 probable secondary COVID-19 cases among 61 participants (85.2%)
An epidemiological investigation at a call centre in South Korea showed an attack rate of 43.5% among 216 employees on the 9th floor of the call centre indicating high transmission in crowded indoor workplace environment. Most of the infected employees were sitting at the same side of the 9th floor which suggests the influence of proximity, but there was no obvious relation of risk of transmission and distance from the index case on this side of the 9th floor. The authors also conclude that the duration of contact played the most important role in spreading of COVID-19, since the cases were limited almost exclusively to the 9th floor despite interaction with colleagues in other settings (such as the elevators and lobby).
It is not possible to disentangle in these reports the role of physical proximity and direct contact through handshaking, or indirect transmission through contaminated objects and surfaces or longer distance transmission through aerosols. However, they illustrate the risk of transmission in crowded indoor settings and the importance of bundled prevention measures.
A systematic review and meta-analysis of 172 observational studies both in healthcare settings and the community, that looked into the effect of distance from the source patient and the use of respiratory and eye protection in the risk of transmission of SARS-CoV, MERS-CoV and SARS-CoV-2, concluded that physical distancing of at least one metre, use of face masks and eye protection were associated with a much lower risk of transmission. Distances of two metres provided an even larger protective effect and the use of respirators was found to be more protective than medical masks in this review.
In a restaurant outbreak of 10 cases in three families in Guangzhou, China, transmission was attributed to the spread of respiratory droplets carrying SARS-CoV-2 by the airflow generated by the air-conditioning.
Similarly, two other outbreaks from China in January 2020 attribute air conditioning systems using a re-circulating mode as a likely aid to transmission.
ECDC guidance is much more in tune with the emerging scientific consensus around the three routes of transmission being very likely, and the need to take measures against all of them, especially in enclosed indoor spaces.
7. Specific outbreak events
We will now look at some of the reports of specific outbreak events, starting with those mentioned in the ECDC guidance
Choir in Washington State
This outbreak in March 2020 clearly points to aerosol spread being involved. The choir of 61 people sang for 2 ½ hours, inside an enclosed rehearsal hall which was roughly the size of a volleyball court (about 160 m2). Even though people were aware of the virus and took steps to minimize transfer of virus; e.g. they avoided the usual handshakes and hugs hello, there was hand sanitiser at the door, people also brought their own music to avoid sharing. Social distancing was apparently not rigorously followed however during the practice session. The organisers also told choir members prior to the session that anyone experiencing symptoms should stay home. One person who had cold-like symptoms infected most of the people in attendance. The long period of time of exposure, the enclosed space and the forceful breathing during singing by everyone ensured that almost everyone became infected Over a period of 4 days, 53 of the 61 choir members became infected, and two died. (28) (41)
Work of breathing is important. Indoor spaces where people are physically active with increased work of breathing promote spread for two reasons: firstly, more virus is expelled from people who are infected, and secondly, increased rate and depth of breathing by non-infected people draws in much more air into the lungs, and with it any virus in the surrounding air. Indoor fitness centres with poor ventilation are therefore potentially very hazardous for spread; people doing vigorous workouts breathe in and out approximately 20 times the volume of air per minute compared with quiet breathing.
Restaurant in Guangzhou
A report of an outbreak of Covid-19 in a restaurant in Guangzhou in late January and early February also demonstrates likely aerosol spread, from a single asymptomatic carrier in a restaurant environment. The seating arrangements are shown below. The infected person (A1) had dinner with 9 friends. During the meal, which took about an hour, the asymptomatic carrier released low-levels of virus into the air from breathing. Airflow, from various airflow vents, was from right to left. The tables were about 1 metre apart. About half the people at the infected person’s table became sick over the next seven days. 75% of the people on the adjacent downwind table became infected. Two of the 7 people on the upwind table were infected (probably by turbulent airflow). No one at tables E or F became infected, they were out of the main airflow from the air conditioner on the right to the exhaust fan on the left of the room. (29)
Incidentally this outbreak demonstrates quite clearly that sitting back-to-back in an indoor environment does not offer protection from infection. Direction of airflow is important.


Seating at Guangzhou restaurant showing location of index case and those subsequently infected. This is one part of a larger space which had another air conditioning unit.
Call centre in Seoul
Another informative and thorough study (30) was of an outbreak in a call centre in early March in Seoul, South Korea (see figure below). A single infected employee worked on the 11th floor of a building; that floor had 216 employees. Employees did not generally move between floors, and they did not have an in-house restaurant for meals. Over the period of a week, 94 of those people became infected (43.5%: the blue chairs in the figure). Three other people on different floors were also infected. Note how one side of the office was mainly infected, but there were others at some distance away on the other side, who also became infected. While the number of people infected by different routes, i.e. respiratory droplets, aerosol or fomite transmission (door handles, shared water coolers, elevator buttons etc.) is unknown, this shows that being in an enclosed space, in a crowded office environment and sharing the same air for a prolonged period is very high risk for exposure and infection.
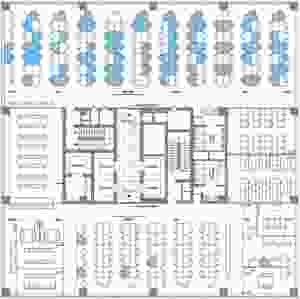

Floor plan of the 11th floor of building X, site of a coronavirus disease outbreak in Seoul, South Korea, March 2020. Blue colouring indicates the seating places of persons with confirmed infection.
Interestingly, even though there was interaction with other people on different floors of the building in elevators and the lobby, the outbreak was almost entirely limited to a single floor, which indicates that the duration of interaction (or contact) was likely the main reason for further spread.
This clearly has implications for office working while the rate of infection in the community is high, as in the UK at present. This seems to already be happening, a Guardian article dated 2 July 2020, reported that suspected outbreaks of Covid-19 in English workplaces had doubled in the space of a week. (38)
TRANSMISSION ON BUSES
Bus drivers in London
Recent Office of National Statistics (ONS) figures showed that bus and coach drivers have 2.5 times the average death rate from Covid-19.(31) At least 33 bus drivers have died of Covid-19 in London. (32)There are no studies to determine which route of spread is responsible but if we look at what happens on a London bus, we can get a good idea.
Passengers board at the front door, “touch in” using a card reader in front of the driver and then move into the bus and sit down. The driver is separated by a Perspex screen, with small holes in it, from the passengers, and there is no hand to hand contact as paying for fares has been cashless since 2014. The contact time between passengers and the driver is very short – a few seconds, so it is highly unlikely that an infective dose of virus could be passed to the driver by passengers touching in and then taking a seat. Passengers are not allowed to stand near the driver during travel, and while one or two passengers may talk to the driver when boarding this is infrequent and for 1-2 minutes at most. If an infected person coughed or sneezed, straight at the Perspex screen without covering their mouth and nose then conceivably enough virus could be transmitted to the driver to cause infection. This however is an unlikely and very infrequent event.
So if surface contact spread is unlikely (there are few opportunities for shared contact surfaces between passengers and the driver), and the large droplet route of spread is unlikely due to very brief contact times, this leaves aerosol spread as the likely culprit.Average daily commuting journeys by bus are about 40-45 minutes each way according to the Trades Union Congress (10 minutes longer for BAME people) (33), so an infected passenger will be breathing virus into the air inside the bus for this period.The passenger may be talking, coughing or laughing, producing more virus. There may be more than one infected passenger on board at any one time and over the course of a working day several passengers with Covid-19 may travel on the same bus with the same driver.
For some weeks Transport for London closed the front doors on buses in an effort to reduce exposure for the drivers. But as discussed, close contact time is very short, making it very unlikely that enough virus would be spread to the driver. This measure has now been withdrawn, and numbers of passengers restricted, and face masks made compulsory for passengers, which should make a significant difference.
However, ventilation on London buses is poor. As can be seen from the photograph below, there are two small windows high up on each side, and while air will circulate when the doors are opened, the air soon becomes still again when they are closed again. Restrictions are now in place on the number of passengers allowed on each bus; 10 downstairs and 10 upstairs. The space is small however, favouring diffusion of virus throughout the air. One bus driver stated he thought the reason so many of his colleagues died was “We are in a capsule with all that Covidy air circulating around us.” (32)


Bus passengers in Zheziang
Airborne spread on buses is also supported by a preprint study by Shen and Li in April 2020 of an outbreak on a bus trip in Zheziang, China. This showed that distance from the index patient on the bus did not make any difference to pattern of infection.23 of 67 passengers became infected – see diagram below.
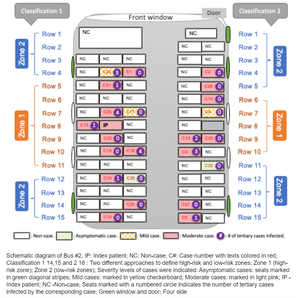

The authors state,
“Our data strongly suggest that airborne transmission contributed to the COVID-19 outbreak. …. The buses had an air conditioning system on a re-circulating mode, which may have facilitated the spread of the virus….. If COVID-19 transmission occurred solely through close contact or respiratory droplets during this outbreak, risk of COVID-19 would likely be related to distance from the index case and ‘high-risk’ zones on the bus would have more infected cases……. Our findings suggesting airborne transmission of COVID-19 is in line with a past report of a SARS outbreak on a plane (discussed above). In closed environments with air re-circulation, COVID-19 is a highly transmissible pathogen. Our finding of likely airborne transmission has important public health significance (for) future efforts at prevention and control.” (34)
Transmission in meat and poultry processing plants
There have been widespread outbreaks of Covid-19 in this industry, in several countries. In the US by 25 June, 25,000 meat and poultry workers had been infected and there were at least 91 deaths (35) There have been large outbreaks in Germany, France, Spain, Holland, Brazil, Australia, and recently in the UK. In West Yorkshire 150 out of more than 500 workers became ill with the virus in June in the Kober plant, 58 workers became infected in Anglesy in the 2 Sisters plant. Three workers died in May at another meat processing plant in South Yorkshire.
Various reasons for these outbreaks have been put forward.Company owners say they observe strict distancing and hygiene measures (35), if this is true it suggests neither droplet or contact spread is the main reason.Others point to crowded spaces like locker rooms and shuttle buses, and shared accommodation.Workers in this industry are often poorly paid and on short term precarious contracts, resulting in pressure to remain at work even if ill, and therefore act as sources of infection.The Guardian reported that a family member of one worker who had died said they only received statutory sick pay of £95.85 a week, and no other support. (36).
The timing of the outbreaks however points to aerosol spread being involved, i.e. a large number of people being infected within a few days of each other, typical of so called “super spreader events” among people sharing the same indoor space for many hours. These plants are deliberately kept cold, which favours Covid-19 survival, there is noisy machinery so workers often have to shout to communicate, meaning lots more virus in the air. Ventilation may be inadequate in many of the plants; the CDC recommended that the companies should ensure “adequate ventilation that minimizes air from fans blowing from one worker directly at another worker.” (36)


The photograph illustrates the working conditions in one meat packing plant in the US; With thanks to The Counter: https://thecounter.org/meat-processing-plant-covid-19-cdc-report-coronavirus/ See here for other pictures: https://images.app.goo.gl/fYZ4t5xBWcjMGxTr8
It is not difficult to see how one or two infected workers might spread the virus throughout this large busy environment over the course of a few hours. Other plants have plastic sheeting hung between workers on the production line, but ventilation is still the fundamental issue in an enclosed environment like this, even if the number of workers present is reduced.
On 25 June the Guardian reported that in Germany the air filtration system had probably contributed to one large outbreak.
“Martin Exner, a hygiene and public health expert at the University of Bonn, analysed the Tönnies meat packing plant in Gütersloh, a western German city sent back into lockdown this week after around 1,500 employees were infected with coronavirus. Exner said the air filtration system in the slaughter area had contributed to the spread of aerosol droplets laden with the virus, ……. The area of the plant where animals are slaughtered, gutted and cut to pieces is kept at a cool 6-10C degrees. To do this, the cooling system circulated the same unfiltered air, thus keeping aerosols in motion, Exner said. A filter fitted to the cooling system was not able to keep out the virus, his analysis found.” (37)
Other publications and reports
There are a wide range of other reports clearly pointing to aerosol spread of Covid-19, from reputable authors and journals. Rather than discussing them in detail here, they are listed below under “Other publications” with a brief excerpt from each.
8. A word about face coverings
While this article is not about protective measures against Covid-19, given the controversy about face coverings it is worth restating they are very effective and are an essential weapon in the fight against the virus. They work because they reduce aerosol spread by trapping the tiny droplets containing virus as they leave the mouth and before they evaporate and the viral particles become suspended in the air, i.e. aerosolise. A recent paper in the Annals of Internal Medicine states, “Cloth does not stop isolated virions (virus particles). However, most virus transmission occurs via larger particles in secretions, whether aerosol (<5 µm) or droplets (>5 µm), which are generated directly by speaking, eating, coughing, and sneezing; aerosols are also created when water evaporates from smaller droplets, which become aerosol-sized droplet nuclei. The point is not that some particles can penetrate but that some particles are stopped, particularly in the outward direction. Every virus-laden particle retained in a mask is not available to hang in the air as an aerosol or fall to a surface to be later picked up by touch.” (39)The paper goes on to say, in the fight against this deadly pandemic every tool we have should be used.


Kimberly A. Prather et al. Science 2020;368:1422-1424
Each day it seems there is a new paper demonstrating the effectiveness and importance of face coverings for the general public. This recent paper from Zhang et al in the Proceedings of the National Academy of Sciences states, “…airborne transmission is highly virulent and represents the dominant route to spread the disease. By analyzing the trend and mitigation measures in Wuhan, China, Italy, and New York City, from January 23 to May 9, 2020, we illustrate that the impacts of mitigation measures are discernable from the trends of the pandemic. Our analysis reveals that the difference with and without mandated face covering represents the determinant in shaping the pandemic trends in the three epicenters. This protective measure alone significantly reduced the number of infections, that is, by over 78,000 in Italy from April 6 to May 9 and over 66,000 in New York City from April 17 to May 9. Other mitigation measures, such as social distancing implemented in the United States, are insufficient by themselves in protecting the public. We conclude that wearing of face masks in public corresponds to the most effective means to prevent interhuman transmission, and this inexpensive practice, in conjunction with simultaneous social distancing, quarantine, and contact tracing, represents the most likely fighting opportunity to stop the COVID-19 pandemic.” (40)
9. Conclusion
The current position of Public Health England, the CDC and the World Health Organisation, on the routes of transmission of Covid-19, is not tenable, and should be amended as a matter of urgency. As we have said the pandemic is accelerating across the world, we have passed the 10 million cases mark and 500,000 deaths. Thousands of organisations across the world look to these world-renowned authorities when they draw up policies and guidance for their employees, members, and the public, and the current advice they depend on, is inherently unsafe, putting millions at risk.
This situation is strongly reminiscent of the weeks of delay and prevarication by all three organisations over advice on wearing facemasks. All three now enthusiastically endorse masks.
The implications for workers, trade unions and members of the public are profound: these bodies are statutory organisations, their guidance is relied upon by the courts and industrial tribunals. Employers and governments reluctant to accede to demands for airborne protections against Covid-19, in particular to ensure proper ventilation in indoor spaces, can and will point to official guidance and say it is not a recognised route of spread and countermeasures are therefore not required.
Quite why these bodies cling to what is now clearly outdated guidance is not clear.The implications of changing the guidance to include airborne spread, are obviously wide- ranging and very challenging, as this effectively means re-evaluating risk in every indoor environment, many of which will not be able to be easily made “covid safe”.
The repercussions of leaving things as they are however, may be far worse.
10. Open letter
If you would like to add your name to an open letter to the heads of WHO, CDC and PHE, calling on them to urgently review their guidance in the light of the evidence, please click here, and share with others. Thank you.
11. Other publications about airborne spread of Covid-19
a) Reducing transmission of SARS-CoV-2
Kimberly A. Prather; American Association for the Advancement of Science 27 May 2020 https://science.sciencemag.org/content/early/2020/05/27/science.abc6197
“…..a large proportion of the spread of coronavirus disease 2019 (COVID-19) appears to be occurring through airborne transmission of aerosols produced by asymptomatic individuals during breathing and speaking (1—3). Aerosols can accumulate, remain infectious in indoor air for hours, and be easily inhaled deep into the lungs.”
b) World Economic Forum report https://www.weforum.org/agenda/2020/04/coronavirus-microdroplets-talking-breathing-spread-covid-19/
“Microdroplets carry many viruses,” says Kazuhiro Tateda, head of the Japanese Association for Infectious Diseases. “We produce them when we talk loudly or breathe heavily. People around us inhale them and that’s how the virus spreads. We’re beginning to see this risk now.”
The report contains a link to an instructive video showing the persistence of droplet nuclei in the air in enclosed spaces, and how ventilation effectively removes them.
c) Is the coronavirus airborne? Experts can’t agree, but a pre-cautionary approach is warranted. Nature 2 April 2020: https://www.nature.com/articles/d41586-020-00974-w
“Aerosols are also more likely to be produced by talking and breathing, which might even constitute a bigger risk than sneezing and coughing, says virologist Julian Tang at the University of Leicester, UK….. The assumption should be that airborne transmission is possible unless experimental evidence rules it out, not the other way around, says Tang. That way people can take precautions to protect themselves.”
d) Small droplet aerosols in poorly ventilated spaces and SARS-CoV-2 transmission
Lancet Respiratory Medicine, 27 May 2020 : https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30245-9/fulltext#back-bib8
The droplets can be transmitted either directly by entering the airway through the air (aerosols), or indirectly by contact transfer via contaminated hands. The mode of transmission could affect whether an infection starts in the upper or lower respiratory tract, which is thought to affect the severity of the disease progression. Notably, the dose–response relationship of SARS-CoV-2 infection is still unclear, especially with respect to aerosol transmission of the virus. However, aerosols containing a small concentration of virus in poorly ventilated spaces, combined with low humidity and high temperature, might result in an infectious dose over time.
e) Airborne transmission of SARS-CoV-2: The world should face the reality.
Science direct 2020. https://www.sciencedirect.com/science/article/pii/S016041202031254X
(While) social distancing and self-isolation ……..have worked well under lockdowns, the potential of airborne transmission of COVID-19 under the eased restrictions has not been considered important enough. We discuss the need to acknowledge the airborne spread of COVID-19 inside built spaces under eased movement restrictions and the potential steps that can be taken to control it.
f) 2019 Novel Coronavirus (COVID-19) Pandemic: Built Environment Considerations To Reduce Transmission.
mSystems, American Society for Microbiology. https://msystems.asm.org/content/5/2/e00245-20
“With the rapid spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that results in coronavirus disease 2019 (COVID-19), corporate entities, federal, state, county, and city governments, universities, school districts, places of worship, prisons, health care facilities, assisted living organizations, daycares, homeowners, and other building owners and occupants have an opportunity to reduce the potential for transmission through built environment (BE)-mediated pathways.”
g) Identifying airborne transmission as the dominant route for the spread of COVID-19
Physical Science, Proceedings of the National Academy of Sciences.11 June 2020
https://www.pnas.org/content/117/26/14857#sec-5
We have elucidated the transmission pathways of coronavirus disease 2019 (COVID-19) by analyzing the trend and mitigation measures in the three epicenters. Our results show that the airborne transmission route is highly virulent and dominant for the spread of COVID-19.
h) Database of 1,100 + Covid-19 Super spreading events (SSE) Blogpost Koen Swinkels: 12 June 2020 . https://medium.com/@codecodekoen/covid-19-superspreading-events-database-4c0a7aa2342b
……the role of aerosols in transmission (should be investigated further). It seems worthwhile to take a closer look at the degree and types of ventilation, air conditioning and humidity control in known SSE settings, as well as at the nature of activities — singing, laughing, shouting and exercising, for example — that took place in such settings
i) Airborne transmission of Covid-19. Occupational Medicine, Oxford Academic. 1 June 2020. https://academic.oup.com/occmed/article/doi/10.1093/occmed/kqaa080/5849370
These observations and findings raise concerns that COVID-19 may spread widely via fine aerosolized droplets
j) Airborne Spread of SARS-CoV-2 and a Potential Role for Air Disinfection
Viewpoint, Journal of the American Medical Association. June 1, 2020. https://jamanetwork.com/journals/jama/fullarticle/2766821
Although clear evidence of person-to-person airborne transmission of SARS-CoV-2 has not been published, an airborne component of transmission is likely based on other respiratory viruses such as SARS, Middle East respiratory syndrome, and influenza. While air sampling for SARS-CoV-2, in a clinical setting, has demonstrated detectable viral RNA, the extent of transmission resulting from airborne particles relative to large respiratory droplets, directly and on surfaces, is not yet known. But if fitted N95 respirators can be justified as a prudent precaution against airborne infection for health care workers with regular exposure to patients with novel coronavirus 2019 (COVID-19) and nonmedical face coverings justified to be worn in public to reduce aerosol spread, should not air disinfection be deployed in intensive care units, emergency departments, waiting rooms, and ambulatory clinics? This approach may be especially important to prevent spread from asymptomatic persons with infection, who may be sources of transmission in selected public settings.
k) Re-thinking the Potential for Airborne Transmission of SARS-CoV-2;
Allen and Marr. Preprints 2020, 20200501266 May 2020 (not peer reviewed) https://www.preprints.org/manuscript/202005.0126/v1
(Note: This paper is worth quoting at length as it is an excellent summary of the evidence, reasoning and implications of aerosol transmission.)
Evidence for the potential for airborne transmission of SARS-CoV-19 continues to accumulate, with important implications for healthcare workers, as well as the general public. Three lines of evidence support this conclusion.
Detection and survival of coronavirus in air
SARS-CoV-2 viral RNA in air has been detected in several studies in hospitals, including at distances greater than 2 m from patients and in outdoor air in crowded areas near a hospital and a department store.i ii iii One study found that the majority of these viruses were associated with aerosols (i.e., microscopic droplets) of diameter 2.5 microns and smaller, which can remain suspended in air for 2 hours or more.i Another detected SARS-CoV-2 in aerosols in the size range of 1-4 microns.iii Furthermore, viral RNA has been detected on the surfaces of an air exhaust outlet and fan, places where direct transfer from an infected person could not occur.iv While these studies assayed viral RNA, the finding that SARS-CoV-2 in fine aerosols (<5microns) has a half-life of 1 hour in terms of infectivity raises the possibility that some airborne virus is infectious.v If we assume that SARS-CoV-2 survives in large droplets, there is no reason to think that the virus would not also survive in aerosols. Previous studies have shown that other viruses survive equally well, if not better, in suspended aerosols compared to large, stationary droplets.vi vii viii
2. Asymptomatic Infectivity
There are reports of asymptomatic transmission of SARS-CoV-2.ix By definition, asymptomatic patients are not coughing or sneezing, which means they are not frequently generating large droplets. Therefore, for these asymptomatic patients, other modes of transmission, namely fomite and airborne, must be occurring. Studies on patients with confirmed influenza infection, show that infectious virus in fine particles can be released by regular breathing and talking, without coughing.x This is of concern because a new preprint shows high shedding of infectious SARS-CoV-2 in the throat pre-symptoms.xi
3. Aerosol physics
While the traditional distinction between “droplet” and “airborne” transmission of infectious disease has been useful for setting guidelines on the use of personal protective equipment, it has also established a false dichotomy in understanding the behavior of viruses in the air. Virus-containing droplets that are released by breathing, talking, and coughing span a continuum of sizes, from 0.01 to hundreds of microns. It is impossible for someone to release “large droplets” (>5 microns) without also releasing smaller ones.xii Thus, transmission that is purported to occur via the spray of large droplets from a cough could in fact be occurring through inhalation of much smaller droplets at close range. In fact, a physics-based simulation suggests that the majority of exposure at close range occurs by inhalation of small droplets rather than by contact with large droplets that land on the mouth, nose, and eyes, unless the people are closer than 30 cm or the droplets are very large.xiii
Conclusion and Implications
Evidence is emerging indicating that, in addition to transmission via large droplets and fomites, SARS-CoV-2 is also transmitted via airborne particles. Recognition of this transmission route is critically important because healthcare workers are experiencing high rates of infection. A shortage of N95 respirators and other personal protective equipment, and lack of administrative and engineering controls addressing airborne exposure, may be contributing factors. More comprehensive guidance on how to protect healthcare workers and the general public should be considered in light of this new scientific evidence.
12. References
1. https://twitter.com/ChrisGiles_/status/12gb75371427336683520
3. https://www.independentsage.org/wp-content/uploads/2020/06/IndependentSage_briefingnumber_forpress.pdfhttps://www.independentsage.org/review-of-scientific-evidence-on-2-metre-versus-1-metre-social-distancing/
4. https://www.medrxiv.org/content/10.1101/2020.04.04.20053058v1.full.pdfhttps://medium.com/@codecodekoen/covid-19-superspreading-events-database-4c0a7aa2342b
5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7264768/
6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2843952/
7. https://www.sciencemediacentre.org/expert-reaction-to-questions-about-covid-19-and-viral-load/
8. https://www.pnas.org/content/117/22/11875
9. https://www.nejm.org/doi/10.1056/NEJMc2004973
12. https://www.nejm.org/doi/full/10.1056/NEJMoa032867#article_letters
13. https://www.nejm.org/doi/full/10.1056/nejmoa031349
14. https://www.cdc.gov/sars/about/fs-sars.html
20. https://www.cebm.net/wp-content/uploads/2014/06/CEBM-Levels-of-Evidence-Introduction-2.1.pdf
21. https://bestpractice.bmj.com/info/toolkit/learn-ebm/what-is-grade/).
22. https://www.cebm.net/covid-19/hand-disinfectant-and-covid-19/
23. https://www.nap.edu/read/25769/chapter/1
27. https://www.ecdc.europa.eu/en/covid-19/latest-evidence/transmission
28. https://www.latimes.com/world-nation/story/2020-03-29/coronavirus-choir-outbreak
29. https://www.wsws.org/en/articles/2020/05/13/lond-m13.html
30. https://wwwnc.cdc.gov/eid/article/26/8/20-1274_article
32. https://www.wsws.org/en/articles/2020/05/13/lond-m13.html
33. https://www.tuc.org.uk/news/annual-commuting-time-18-hours-compared-decade-ago-finds-tuc
39. https://www.acpjournals.org/doi/10.7326/M20-2567
40. https://www.pnas.org/content/early/2020/06/10/2009637117#sec-5
41. https://www.medrxiv.org/content/10.1101/2020.06.15.20132027v1.full.pdf

Great 👍
For us, these may seem like “No Brainers” but maybe it’s not as easy as is seems. Or maybe its just not a real priority.